

The Relationship of Diet and Breathing
An investigation into the possible relationship between diet and breathing; does what we eat affect the way we breathe and does the way we breathe affect the food we choose to eat?
Preliminary findings suggest there is, indeed, a strong correlation between these two activities.
Over the past years, I have been screening all my patients (who visit me primarily for various musculoskeletal problems) for their diet and breathing. The measures I have used are well-established in clinical practice.
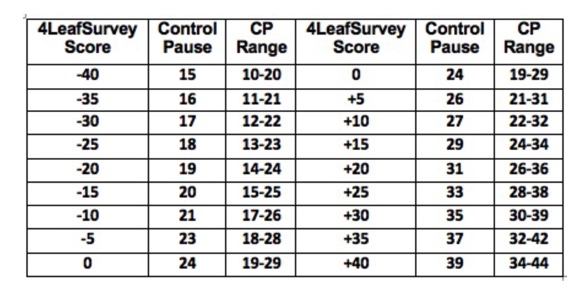
I use the “4Leaf Survey” screening questionnaire to gain a reasonable measure of the percentage of calories the person
derives from whole plant food as opposed to all other foods. This simple twelve-question form is widely used by
doctors in the USA who are advising their patients on Whole Plant Nutrition. The scores range from -40 to +40 and
the table below gives the approximate equivalent percentage of calories from whole plant food.

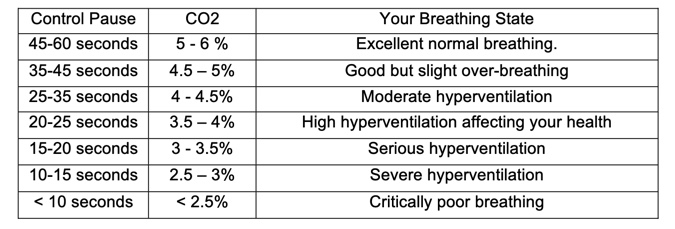
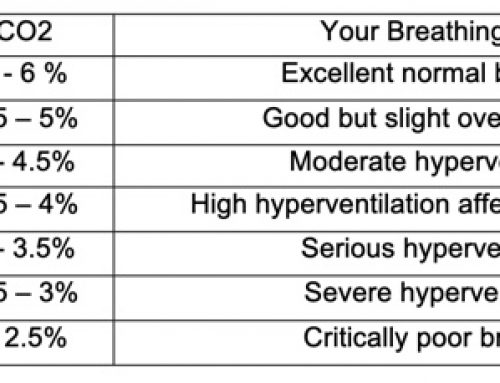
I use the Control Pause to screen for breathing quality; this simple measure was developed by Professor Konstantin Buteyko as part of his breath-training programme. It measures the maximum comfortable breath-hold in seconds, after exhaling while breathing normally at rest.
The scores range from 0 to 60 for the majority of the population. The table below gives the approximate CO2 levels in the lungs and the degree of hyperventilation associated with this measure.
The graph below is based on the results to date of 179 patients:
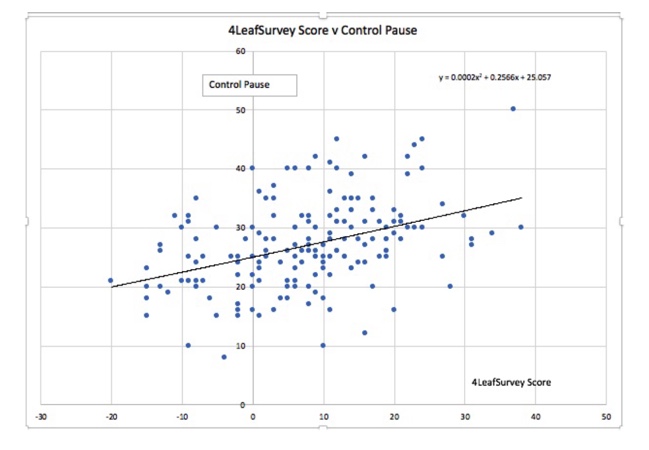
Statistical analysis of these data points gave the following:
CP = 25 + 0.26 x 4LS Score (Standard deviation 5)
Note 47% of all data points are within one SD and 86% are within two SD of mid values.
Statistical analysis of these data points gave the following:
CP = 25 + 0.26 x 4LS Score (Standard deviation 5)
Note 47% of all data points are within one SD and 86% are within two SD of mid values.
There are good physiological reasons why our diet affects our breathing, but why our breathing affects what, and how we eat is more a reflection of psychological factors.
A diet rich in meat, dairy, refined carbohydrates, sugary drinks & processed snacks (the Standard American Diet – SAD) can produce metabolic acidosis. The way the body attempts to correct this can be by drawing calcium from the bones or by excreting more carbon dioxide. The latter is more common as it is also the response to stressors and the fight/flight response with an increased breathing rate. This may be the physiological reason for a low CP when the 4LeafSurvey score is negative and a higher CP when the 4LeafSurvey score is positive.
As regards the possible correlation between breathing and choice of diet, this is more complex. When a person has a high CP (35 to 60 seconds) they are invariably more relaxed and do not suffer much from stress. In this calmer state they are more likely to not want sugary snacks on the run at work, are more likely to take their eating more seriously, sit down to eat at regular meal times, and to choose their food more thoughtfully. In fact, there is only one negative 4LeafSurvey score for all those with a CP over 35. (Under 5%).
There was a relatively low sample of negative 4LeafSurvey scores (18%) compared with what might be found in a SAD diet, this is where I would like to have some input from American Buteyko Educators to get a more reliable picture in this area.
Conclusions:
As a general rule, those studying nutrition do not take account of their patient’s breathing and those studying breathing do not take much interest in their client’s eating habits. Most doctors and therapists have not usually expected any significant link between these two activities.
This preliminary research strongly suggests there is a link that we should further investigate and meanwhile take this into account when offering advice on dietary changes or when providing breath training.
The good news is that it would seem reasonable to expect a person’s breathing will improve if they improve their eating habits and likewise, their eating habits will improve over time if their breathing is improved.
The latter changes may take some time, and in the interim, the patient may be at risk from depleted calcium stores or even the development of kidney stones if the body is left with only this mode of correcting dietary acidosis when breathing has been normalized.
This may also explain why breath-training progress is often slow with those patients on an acid-forming diet.
Michael Lingard BSc. DO. WPNut.Cert.
Orthopath, Buteyko Educator & Plantrician
Email: lingard@totalhealthmatters.co.uk
Web: www.totalhealthmatters.co.uk
Linkedin: www.linkedin.com/in/michaellingard/
Tel: +44(0)1580 752 852
13th October 2018

Leave A Comment